Beyond the Pandemic: AI Contact Tracing System Safeguards Residential Care Homes
Other Articles

An Indoor Bluetooth-Based System Offers a Practical Blueprint for Smarter Infectious Disease Control in Ageing Settings
Study conducted by Prof. Ho Keung David SHUM , Prof. Lin YANGand their research team
, Prof. Lin YANGand their research team
The COVID-19 pandemic changed how the world thinks about infection control, especially in places where vulnerable people live in close proximity. Residential care homes became one of the clearest examples of how quickly an infectious disease can spread when residents share indoor space, require hands-on support and interact regularly with staff and visitors. Even as emergency restrictions have eased, the need for sustainable outbreak preparedness has not disappeared. For the nursing sector, this raises an important question: how can care environments become safer without becoming more restrictive, labour-intensive or intrusive?
A recent study on an AI-empowered indoor digital contact tracing system published in Infectious Disease Modelling [1] offers one possible answer. Prof. Lin YANG, Associate Professor of the School of Nursing at The Hong Kong Polytechnic University, and Prof. Ho Keung David SHUM, Yeung Tsang Wing Yee and Tsang Wing Hing Professor in Neuropsychology and Chair Professor of Neuropsychology of the Department of Rehabilitation Sciences at the same university, together with their research team, developed a system for residential care homes in Hong Kong to monitor indoor movements and contact patterns using low-energy Bluetooth technology, while preserving privacy and minimising disruption to daily life.
More than a COVID-19-specific tool, the study provides practical insights into how smart systems can support outbreak management in ageing services. Its value lies not only in the technology itself, but also in what the collected data reveal about contact patterns, targeted quarantine and the design of more resilient care settings.
The team aimed to develop and test an indoor contact tracing system that could automatically capture high-resolution contact data among care home residents, staff and day-care users. Existing digital tracing approaches have often relied on smartphones, GPS or person-to-person app-based exchanges. These methods can be useful at the population level, but they are less suited to residential care environments. Older adults may not always carry a smartphone, battery consumption can be high and privacy concerns can discourage adoption. In contrast, the system developed by the team used wearable low-energy Bluetooth beacons and fixed gateways placed throughout the care home. This made it possible to track room-level location and overlapping presence in a way that was both more practicable for care settings and less dependent on user behaviour.
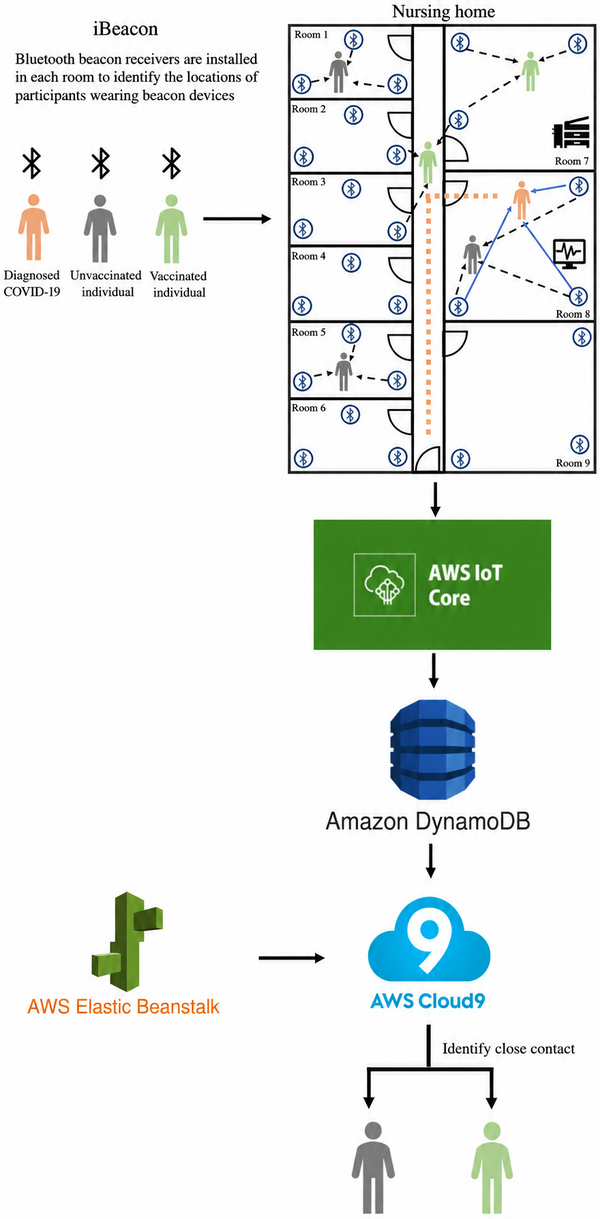
Figure 1. Architecture of the tracing system
The system architecture is particularly relevant for those working at the intersection of ageing, digital health and built environment innovation. It comprised three main components: wearable Bluetooth beacons and indoor gateways for data collection; cloud-based algorithms for processing and localisation; and a web portal for visualisation and operational use (Figure 1).
Each participant wore a small beacon device, available in card or wrist form. These beacons emitted Bluetooth advertisement signals at regular intervals. Gateways installed in rooms received the signals and forwarded them to a cloud server through the MQTT protocol. A minimum of three gateways per room enabled more precise indoor positioning through trilateration. Because the system relied on Bluetooth-received signal strength indication rather than GPS, it was better suited to indoor care environments and consumed far less power. The beacons were lightweight, waterproof and had an estimated battery life of up to three years, making them practical for everyday use.
Once the raw signal data reached the cloud server, localisation algorithms were used to estimate beacon coordinates and timestamps. To improve data quality, the system incorporated calibration, validation and noise reduction. When several gateways received the same beacon signal at the same time, the system identified the most likely room location by selecting the room with the highest number of records. It then converted timestamps into time intervals. If two adjacent timestamps from the same beacon were more than 30 seconds apart, they were not merged into a single interval, reducing the risk of false continuity. Contact duration was determined by searching for overlapping time intervals between different beacons detected by the same gateways. In other words, the system inferred who had shared the same room and for how long.
This processing pipeline matters because outbreak control in care homes is not simply about knowing where people are. It is about understanding patterns of interaction that are otherwise difficult to capture reliably: who spends prolonged time together, how routines differ on weekdays and weekends, and which contact thresholds are most meaningful when identifying close contacts. The web portal translated these data into actionable outputs, including movement paths, lists of high-risk zones and close contacts linked to a confirmed case. For care home managers, such a dashboard could support much faster and evidence-based decisions during an outbreak.
Privacy was a central design principle. The beacon devices did not carry personally identifiable information in the transmitted packets, and the data analysts did not know the identity of beacon users. At the care home level, only designated personnel handling the beacon distribution records could link devices to individuals, while access to contact data was restricted to outbreak situations. This separation between identity management and movement analytics is especially important in ageing services, where trust, dignity and data governance are critical.
The system was tested in two residential care homes in Hong Kong. One was an elderly home with staff, residents and day-care users; the other accommodated both older adults and people with disabilities. Across the two sites, the study collected two weeks of contact data and examined both routine interaction patterns and interactions during an actual COVID-19 outbreak.
The contact analysis showed that indoor interaction patterns varied by user group and by day type. In one care home, residents had longer contact durations with one another than staff did, and some weekday-weekend differences were statistically significant. This suggests that care environments have distinct social rhythms that can shape transmission risk. This is an important reminder that outbreak systems should not merely record contacts. They should also help services understand when and where contact intensity changes over time.
The most compelling findings came from the second care home, where a COVID-19 outbreak occurred during the study period. The index case was identified on one floor, and under the regulations in force at the time, all staff and residents on that floor were transferred to quarantine centres two days later. Within six days, five additional cases were confirmed. In total, six of the 14 residents on that floor tested positive during the outbreak.
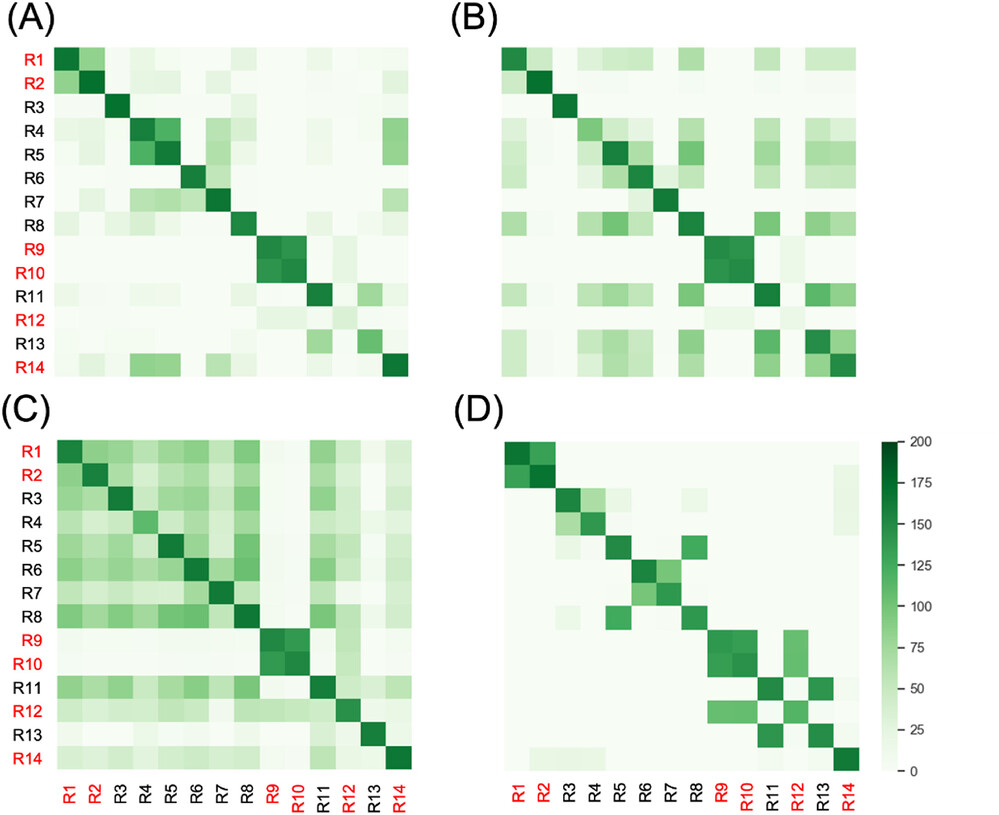
Figure 2. Heat map of daily contact duration (in minutes) between participants (R1 to R14), on (A) the day of the index case diagnosis, (B) one day, (C) two days and (D) three days prior to (A). R14 is the index case. Other numbers highlighted in red are secondary cases. The diagonal line shows the total duration of stay in the residential care home during the exposure period.
The study compared contact durations involving the index case on the day of diagnosis and up to three days prior (Figure 2). Some pairing patterns stood out, such as residents who shared rooms having longer contact durations. However, there was no significant difference between infected and uninfected contacts in terms of demographic characteristics or measured contact duration with the index case. This is a useful caution against assuming that transmission can always be predicted from simple descriptors alone. In real-world care settings, infection risk is shaped by a complex mix of contact time, environmental conditions, host factors and timing within the infectious period.
To explore how the contact data could improve outbreak response, the team built an agent-based simulation model using data from the above outbreak. They compared the real-life strategy of quarantining everyone on the same floor with more targeted strategies based on direct contact with the index case. Thresholds for cumulative contact time were set at 0, 15, 30, 60 and 120 minutes, using either contact on the previous day only or contact over the previous two days.
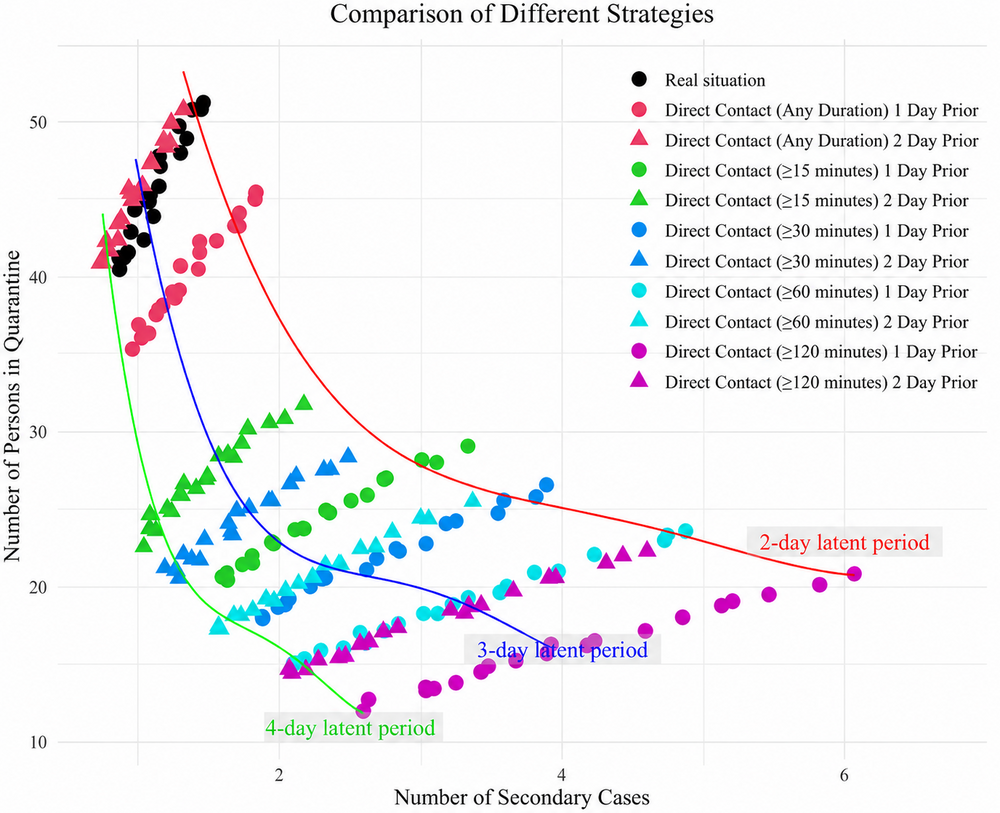
Figure 3. Simulation under different outbreak containment strategies. A multinomial regression line is fitted to the data points under different assumptions of latent period.
The simulation results (Figure 3) are especially relevant for future infectious disease management in care homes. They showed that targeted quarantine based on cumulative contact thresholds one or two days before diagnosis could contain outbreaks much more efficiently than blanket isolation. In particular, thresholds of at least 15 minutes one day before diagnosis and at least 30 minutes one day before diagnosis appeared to mark a turning point: outbreak size could be reduced substantially without quarantining as many people as in a whole-floor approach. In practical terms, this means a better balance between infection control and quality of life. Instead of removing an entire unit from normal activity, services may be able to isolate a smaller group of genuinely high-risk contacts.
This insight has wide implications beyond COVID-19. In care homes, quarantine is never a neutral intervention. It can interrupt routines, increase confusion and distress, reduce social engagement and place an additional burden on staff. A system that enables more selective and evidence-based isolation could therefore support both infection prevention and person-centred care.
The study also highlights several design lessons for future outbreak tracing systems. First, indoor-specific solutions are essential. GPS and mobile apps have limitations in enclosed care environments, whereas room-level Bluetooth systems can capture the kinds of interactions that matter most. Secondly, passive and wearable infrastructure improves feasibility in populations who may not always carry a personal device. Thirdly, privacy-preserving architecture should not be a secondary feature but a prerequisite for implementation in care settings. Finally, tracing systems become more useful when paired with analytics that can translate raw proximity data into actionable thresholds for intervention.
The future of outbreak readiness in care homes will depend on intelligent systems that are practical, privacy-conscious and tailored to indoor living environments. AI-enabled contact tracing can certainly achieve more than document exposure after the fact.
Prof. Shum was recognised by Stanford University as one of the top 2% most-cited scientists worldwide (career-long) in the field of rehabilitation for two years, in 2023 and 2025, and one of the top 2% most-cited scientists worldwide (single-year) for four years, in 2021, 2022, 2023 and 2025. He is a neuropsychologist with 30 years of experience in the assessment and rehabilitation of higher-level cognitive functions in normal and brain-injured children and adults. He has been awarded more than 25 national and international competitive grants from major funding bodies, including the Australian Research Council, the National Health and Medical Research Council in Australia, the Hong Kong Research Grants Council and the Health and Medical Research Fund in Hong Kong. In addition to his university appointments, Prof. Shum currently serves as a member of the Hospital Authority Board, the Chairman of the Hospital Governing Committee of the Pamela Youde Nethersole Eastern Hospital, the Chairman of the Regional Advisory Committee of the Hospital Authority, and a member of the Allied Health Professions Council.
Prof. Yang was recognised by Stanford University as one of the top 2% most-cited scientists worldwide (single-year) in the field of microbiology in 2022. Her research interests include infectious disease epidemiology and infection control and pandemic preparedness, and AI applications in healthcare.
This study, in which Prof. Shum serves as the Principal Investigator and Prof. Yang as the Co-PI, was supported by the Health and Medical Research Fund, the Health Bureau, the Government of the Hong Kong Special Administrative Region.
| References |
|---|
[1] Meng, J., Liu, J. Y. W., Yang, L., Wong, M. S., Tsang, H., Yu, B., Yu, J., Lam, F. M.-H., He, D., Yang, L., Li, Y., Siu, G. K.-H., Tyrovolas, S., Xie, Y. J., Man, D., Shum, D. H. K. An AI-empowered indoor digital contact tracing system for COVID-19 outbreaks in residential care homes, Infectious Disease Modelling, Volume 9, Issue 2, 2024, Pages 474-482, ISSN 2468-0427, https://doi.org/10.1016/j.idm.2024.02.002.
 | Prof. Ho Keung David SHUM |
 | Prof. Lin YANG School of Nursing |


