Beyond the Hype: Older Adults' Perspectives on Smart Healthcare in Hong Kong
Other Articles

What Interview Findings Reveal about Design, Adoption and Support
Study Conducted by Prof. Yan Tina LUXIMON  and her research team
and her research team

As Hong Kong's population ages, smart healthcare technologies (SHCTs) are increasingly seen as part of the answer to rising health and care needs. Wearables, health monitoring stations and mobile health apps are already being promoted to help older adults manage chronic conditions, stay active and access services more efficiently. However, market availability does not necessarily mean meaningful adoption. Real-life use depends on whether these tools are understandable, affordable and relevant in everyday life.
In an exploratory interview study published in Gerontology [1], Prof. Yan Tina LUXIMON, Associate Dean and Professor of the School of Design at The Hong Kong Polytechnic University, and her research team examined how older adults in Hong Kong actually experience SHCTs in practice. Rather than focusing on intention to use, it explored what they are already using, what needs these technologies meet, what barriers remain and what kinds of support make adoption easier.
The study found that older adults in Hong Kong are already using SHCTs, especially to support physical health. Three types were featured most often: smart wearable devices (SWDs), smart health monitors (SHMs) and healthcare applications (HCAs). Five main needs emerged: health monitoring, fall risk management, health information management, convenient access to medical services and maintaining social engagement.
In practice, current technologies were used mainly for physical rather than mental health. The study also identified four main barriers to adoption: technological, personal, financial and informational. At the same time, community-based support, especially from elderly centres, played a major role in reducing those barriers and helping older adults use technologies with more confidence.
The research was based on face-to-face semi-structured interviews with 22 older adults in Hong Kong, with an average age of around 73. Most were living independently, although the majority were managing at least one chronic condition. All had used at least one form of SHCT. This is important in itself: the issue is not whether older adults are using smart healthcare at all, but how well current technologies fit into their lives.
Physical health is where SHCTs currently work best
The clearest finding in the study is that SHCTs are mainly supporting physical health management. Participants used health monitoring stations, wearables and apps to track indicators such as blood pressure, weight, step count and general activity levels (Purple bars in Figure 1). For many, this offered practical support for self-management. Monitoring was not simply about collecting data; it helped users notice changes, adjust routines and stay more aware of their health.
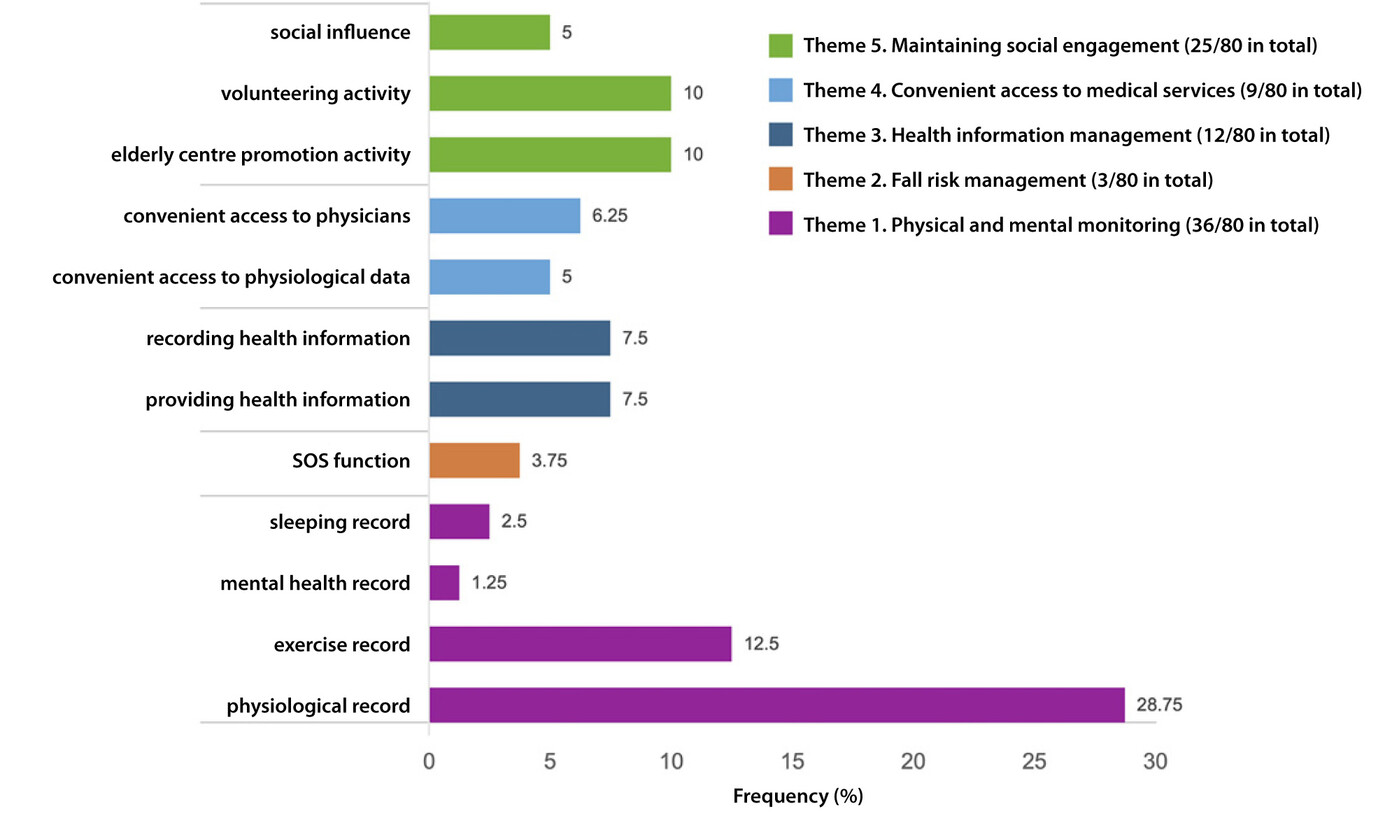
Figure 1. Frequency of themes (five types of real-life needs for healthy ageing) and 12 sub-themes as percentages of the number of responses (80 in total)
For some, the value also came from follow-up by community staff (Green bars in Figure 1). Where an elderly centre was involved, readings could trigger a check-in or enquiry to seek further care. This made the technology connected to in-person support rather than it operating in isolation—the benefit came not only from the device itself, but from the surrounding service and social context.
Activity tracking was another valued feature (Deep blue bars in Figure 1). Step counts, exercise goals and simple forms of comparison with peers helped some participants stay motivated. This suggests that older adults do not only value SHCTs for clinical monitoring; they also appreciate tools that encourage healthier everyday habits.
Fall risk and emergency support matter, but are often adopted late
Fall risk management emerged as an important need, particularly through emergency alert functions in wearable devices. However, the study suggests that adoption in this area is often reactive (orange bar in Figure 1). Many older adults only began using such technology after a fall or health incident, rather than beforehand as a preventive measure.
This points to a mismatch between recognised value and real uptake. Emergency functions are clearly meaningful, especially for those living alone or seen as physically vulnerable. However, concerns about cost, comfort or device design can delay adoption until after a crisis has already occurred.
Healthcare apps are most useful when they solve everyday problems
Healthcare applications were mainly used for managing practical information: appointment records, medical account details, medication records and allergy histories. These are not dramatic uses of technology, but they are highly relevant. They help older adults navigate the healthcare system more smoothly and communicate more effectively with clinicians.
This matters for the smart ageing sector because it shows that usefulness does not always depend on advanced functions. In many cases, technologies become valuable when they remove small but recurring frictions in daily care management.
Interest in convenient medical access is growing
Participants also expressed interest in more convenient access to healthcare, particularly online consultations or rapid digital contact with professionals. Although face-to-face care remained the preferred mode for many, the appeal of immediate reassurance was clear, especially in situations involving uncertainty about medication or symptoms.
Yet the study found that such services were still not common or well-tailored to older adults in Hong Kong. This suggests an area of opportunity for service providers and designers: not to replace in-person care, but to supplement it with age-friendly digital access where appropriate.
Mental health remains a clear gap
One of the most significant findings is what current SHCTs are not doing. While participants used technology for physical health in multiple ways, there was far less evidence of technology supporting mental health. This is striking given that some participants reported anxiety or low mood. The study argues that current SHCTs in Hong Kong still do not adequately address mental health needs in later life. This is a crucial message for both researchers and industry. Healthy ageing is not only about monitoring blood pressure or counting steps. Emotional wellbeing, loneliness and social connection are equally important, yet current solutions appear limited in these areas.
The study identified four categories of barrier, showing that adoption problems are not just technical. The responses are illustrated in Figure 2.
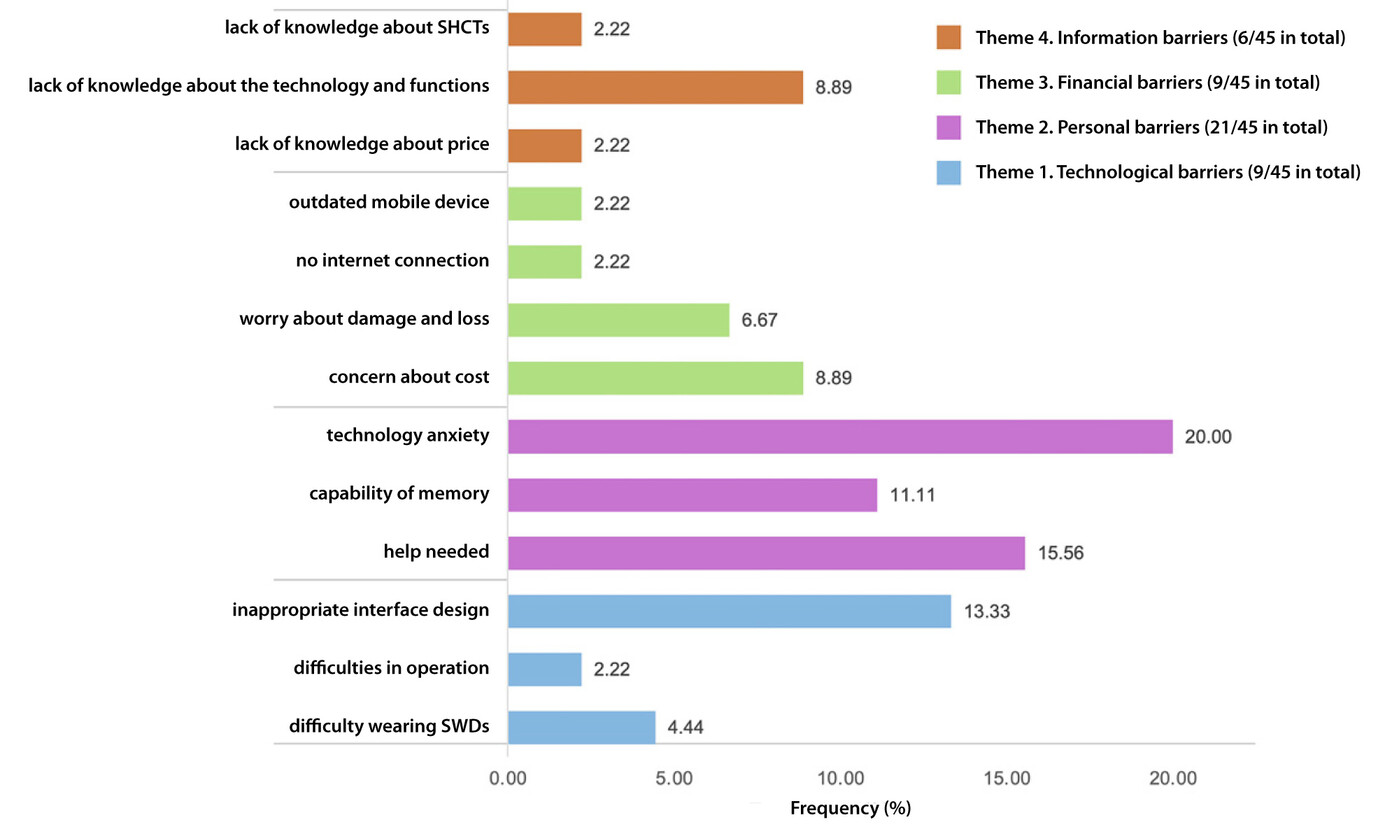
Figure 2. Frequency of themes (four types of barriers) and sub-themes as percentages of the number of responses (54 in total)
Technological barriers
Participants often struggled with small buttons on wearables, small icons and font sizes in apps, and interfaces that were difficult to learn. By contrast, fewer barriers were reported for the smart health monitors placed in elderly centres, likely because these were designed to be more user-friendly for older adults, with simple navigation and clear displays.
This comparison reinforces an important point: age-inclusive design makes a decisive difference. Where design more closely addresses users’ cognitive and physical needs, barriers fall noticeably.
Personal barriers
Many participants reported technology anxiety, even when they had already gained some digital experience. They worried about making mistakes, damaging a device or not being able to learn how to use it properly. A brief training session was often not enough to build the level of confidence needed for continued independent use.
One participant captured this clearly: "I didn't know how to use (SWDs). I was afraid that I would damage it, which is a waste of money." This reflects a wider issue of confidence, not simply competence.
Financial barriers
Cost concerns were also common. Some older adults assumed SHCTs would be expensive before even trying them. Others faced indirect access problems: old smartphones, limited internet access or reliance on free Wi-Fi in community settings. Thus, affordability is not just about device price, but about access to the wider digital infrastructure needed to use these tools reliably.
Information barriers
A further obstacle was lack of awareness. Some participants did not know what technologies existed, what they could do or how much they actually cost. In some cases, they described needs that existing technologies might already address, but they had never been introduced to those options. This highlights the importance of outreach, demonstration and trusted information channels.
One of the strongest messages from the study is that successful adoption depends heavily on social support. Elderly centres in Hong Kong were especially important in providing training, encouragement and opportunities for peer learning. In some cases, older adults became volunteers helping others use the technologies, which strengthened both their own confidence and their social engagement. This helps explain why smart health monitors in community settings were experienced more positively than wearables or apps used more independently. Good design mattered, but so did having ongoing support nearby.
Family support also played a role, though often in a more limited way, such as helping with setup. The findings suggest that smart ageing initiatives work best when technology is embedded in a supportive local ecosystem rather than left to individuals alone.
The study provides a valuable reality check for the smart ageing field. Older adults in Hong Kong are using SHCTs in meaningful ways, especially for physical health monitoring, activity tracking and practical healthcare management. At the same time, current technologies still fall short of effectively addressing older adults’ wider needs, particularly in relation to mental health.
The findings show that adoption is shaped by a combination of design, confidence, cost, information and social context. Effective smart healthcare must be usable, affordable and clearly relevant, but it must also be supported by community structures that help older adults learn, trust and continue using it. If smart healthcare is to contribute fully to healthy ageing, it must be fit for real life, not just technological ambition.
Prof. Luximon is Leader of the Asian Ergonomics Design Lab and Chair of the School of Design Research Committee. She has published over 150 peer-reviewed journal papers, books, book chapters, patents and international conference papers. Her research interests include ergonomics in design, anthropometry and its application in design, 3D digital human modelling and CAD, AI design tool and visualisation, head and face related products, human computer interaction, cultural difference, and statistical and mathematical models. Her ergonomic designs have earned her several international awards, including a gold medal with congratulations of the Jury in the 49th International Exhibition of Inventions of Geneva in 2024 and a silver award in the International Design Excellence Awards 2023.
| References |
|---|
[1] Zhang, J., Wang, H., Li, Q. & Luximon, Y. (2024). What Is the Real-Life Experience of Older Adults on Smart Healthcare Technologies? An Exploratory Interview Study, Gerontology (2024) 70 (9): 978-990. DOI: 10.1159/000539539
 | Prof. Yan Tina LUXIMON Associate Dean (Research) and Professor, |


