
What is Adolescent Idiopathic Scoliosis (AIS)?
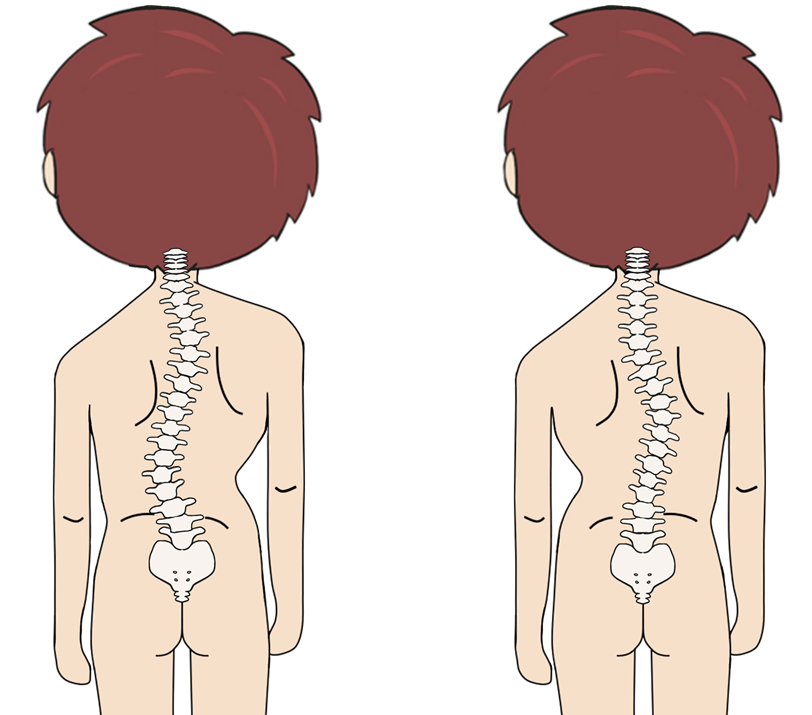
Scoliosis is a condition with abnormal lateral curve of the spine, usually in an elongated C or S shape and vertebral rotation. Adolescent Idiopathic Scoliosis (AIS) is the most common type of scoliosis, which involves about 2-3% of adolescents with unknown cause [1,2]. The ratio of female to male is around 8:2. The major risk factors for scoliosis may include family history, and female with age between 10 to 15 [3].
The onset of AIS in children is around the age of 10 and it can progress rapidly during puberty. The diagnosis of scoliosis can often be overlooked or delayed as most patients remain asymptomatic. However, some patients may develop various complications, that affect their physical, social and psychological wellbeing. The major complications of scoliosis involve impaired cardiopulmonary function, chronic back pain, body image disturbance such as uneven shoulders, prominent ribs and asymmetric trunk [4,5].
Progression of Scoliosis
The progression of scoliosis is determined by the curve magnitude and growth potential [6, 7].
1. Curve Magnitude
The severity of scoliosis depends on the magnitude of spinal curve. This is measured by Cobb angle, which is generally used to quantify the magnitude of spinal deformities [8].
Evidence showed that the risks of spinal deformity progression increase with a higher initial magnitude of spinal curve [9,10]. According to a study that involved 186 skeletally immature patients with idiopathic scoliosis, it was found that the initial magnitude of spinal curve is the most important predictor for long-term spinal deformity progression [10,11].
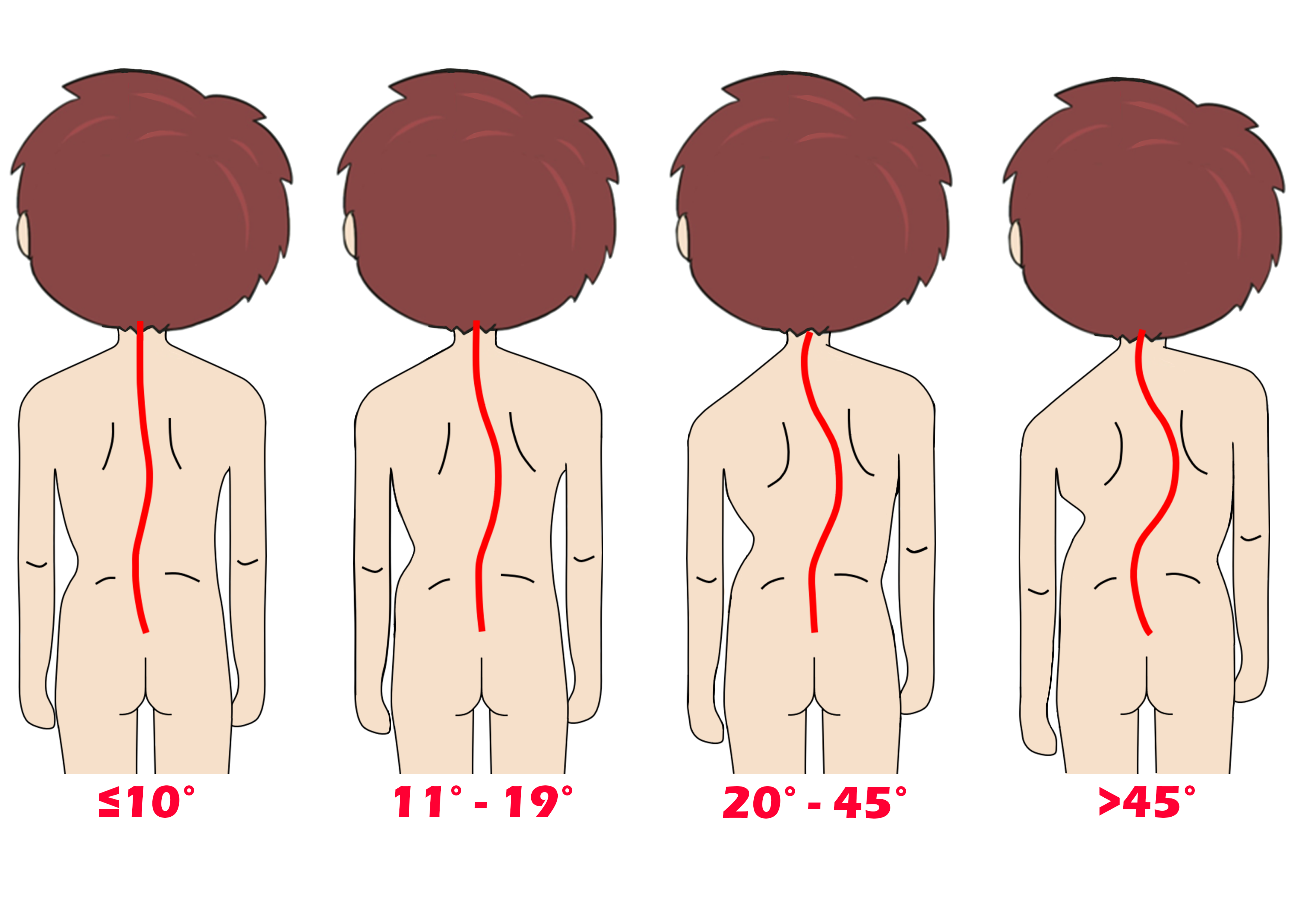
Different magnitudes of spinal curve
2. Growth Potential
Scoliosis usually progresses rapidly in growth period, and the growth potential can be assessed by body height, secondary sexual characteristics, the status of females’ menstrual period (female cases) and the bone age (the degree of maturity of a child’s bone, usually can be assessed through hand X-ray).
Body height will increase rapidly during puberty, so clinicians can monitor one’s height to estimate his/her growth potential. Generally, girls grow until 14 years old, and boys grow until age of 16 [12,13].
In addition, the appearance of secondary sexual characteristics, such as growth of pubic hair, enlargement of breasts in females and enlargement of larynx in males, indicates the onset of puberty period [14]. Also, girls grow very fast until their first menstrual period, and grow slower afterwards. Adolescents usually continue to grow until approximately 2 years after their first menstrual period [15].
Clinicians can also estimate growth potential using the "Risser’s sign grade”, which measures bony fusion of the iliac apophysis. A higher Risser’s sign grade indicates a greater skeletal ossification (increase in maturity from grade I to V), hence, less potential for growth and spinal deformity progression [16,17].
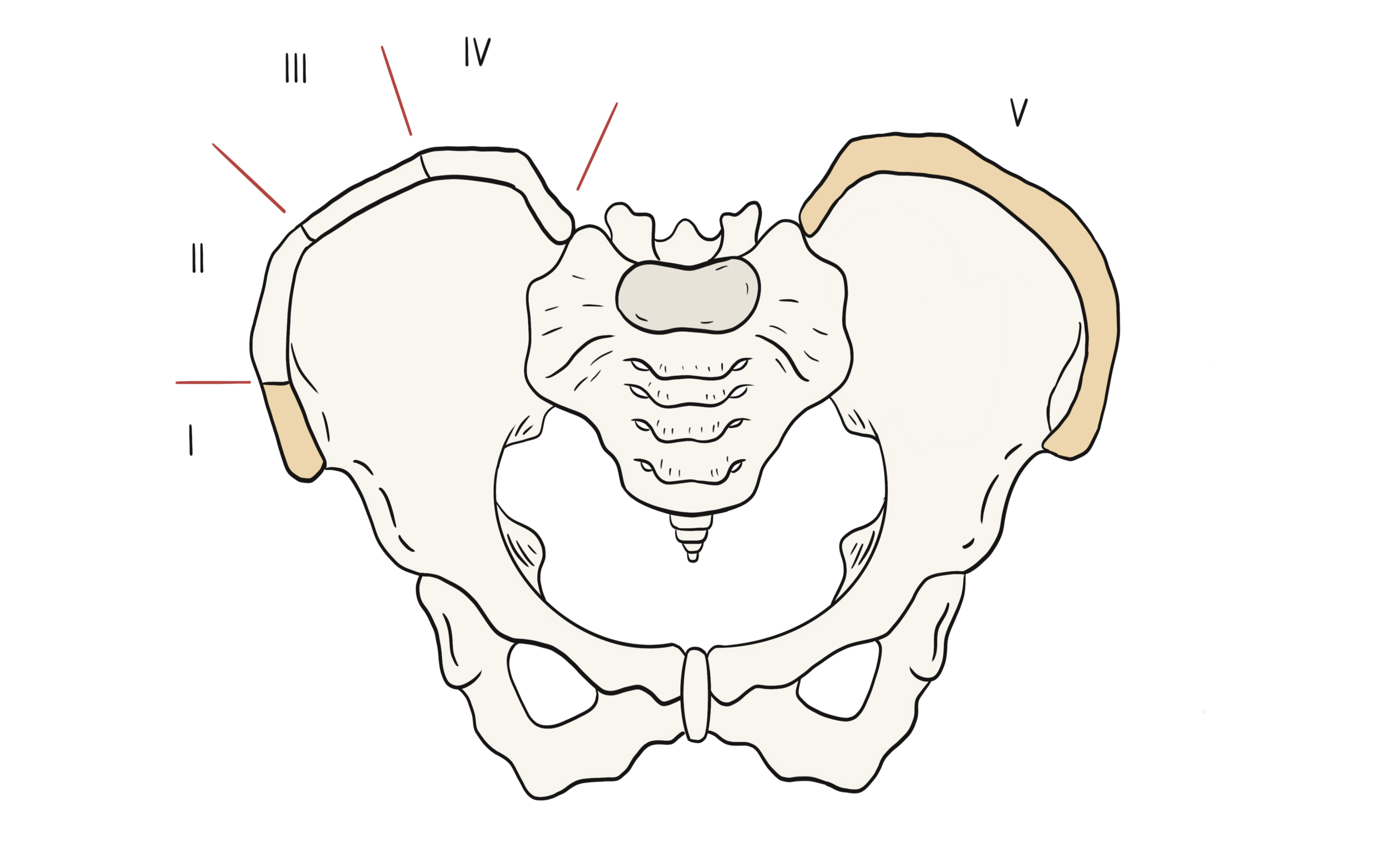
Risser’s sign grade
In conclusion, the risk of spinal deformity progression increases with a larger curve magnitude and higher growth potential (less mature).
Reference
-
SRS. "Scoliosis Research Society." https://www.srs.org/patients-and-families/conditions-and-treatments/adolescents.
-
J. Dubousset, "Definition of Adolescent Idiopathic Scoliosis," in Pathogenesis of Idiopathic Scoliosis: Springer, 2018, pp. 1-25.
-
J. R. Smith, D. M. Sciubba, and A. F. Samdani, "Scoliosis: a straightforward approach to diagnosis and management," Journal of the American Academy of PAs, vol. 21, no. 11, pp. 40-48, 2008.
-
M. Clinic. "Scoliosis." https://www.mayoclinic.org/diseases-conditions/scoliosis/symptoms-causes/syc-20350716.
-
S. H. Service. "Scoliosis." https://www.studenthealth.gov.hk/english/health/health_bsh/health_bsh_sco.html.
-
J. P. Horne, R. Flannery, and S. Usman, "Adolescent idiopathic scoliosis: diagnosis and management," American family physician, vol. 89, no. 3, pp. 193-198, 2014.
-
Y. P. Charles, J.-P. Daures, V. de Rosa, and A. Diméglio, "Progression risk of idiopathic juvenile scoliosis during pubertal growth," Spine, vol. 31, no. 17, pp. 1933-1942, 2006.
-
J. Cobb, "Outline for the study of scoliosis," Instr Course Lect AAOS, vol. 5, pp. 261-275, 1948.
-
J. Lonstein and J. Carlson, "The prediction of curve progression in untreated idiopathic scoliosis," J Bone Joint Surg, pp. 1061-71, 1984.
-
S. Weinstein and I. Ponseti, "Curve progression in idiopathic scoliosis," The Journal of bone and joint surgery. American volume, vol. 65, no. 4, pp. 447-455, 1983.
-
P. N. Soucacos, K. Zacharis, K. Soultanis, J. Gelalis, T. Xenakis, and A. E. Beris, "Risk factors for idiopathic scoliosis: review of a 6-year prospective study," Orthopedics, vol. 23, no. 8, pp. 833-838, 2000.
-
J. Tanner, R. Whitehouse, W. Marshall, and B. Carter, "Prediction of adult height from height, bone age, and occurrence of menarche, at ages 4 to 16 with allowance for midparent height," Archives of disease in childhood, vol. 50, no. 1, pp. 14-26, 1975.
-
W. A. Marshall and J. M. Tanner, "Variations in the pattern of pubertal changes in boys," Archives of disease in childhood, vol. 45, no. 239, pp. 13-23, 1970.
-
F. Martini, J. L. Nath, E. F. Bartholomew, W. C. Ober, C. E. Ober, K. Welch, and R. T. Hutchings, Fundamentals of anatomy & physiology. Pearson Benjamin Cummings San Francisco, CA, 2006.
-
B. A. Spear, "Adolescent growth and development," Journal of the Academy of Nutrition and Dietetics, p. S23, 2002.
-
M. Wajchenberg, N. Astur, M. Kanas, and D. E. Martins, "Adolescent idiopathic scoliosis: current concepts on neurological and muscular etiologies," Scoliosis and spinal disorders, vol. 11, no. 1, p. 4, 2016.
-
M. Ylikoski, "Growth and progression of adolescent idiopathic scoliosis in girls," Journal of pediatric orthopaedics B, vol. 14, no. 5, pp. 320-324, 2005.