
Treatments
Treatment of adolescent idiopathic scoliosis is determined by various factors [1]:
- Chronological age
- Bone age
- Degree of curvature
- Location of curve in the spine
- Status of menses/puberty
- Gender
- Associated symptoms such as back pain or shortness of breath
A Cobb angle larger than 10° is regarded as the minimum angulation to define scoliosis (view more…). The management options are listed below [2]:
Mild case (Cobb angle = 11° - 19°)
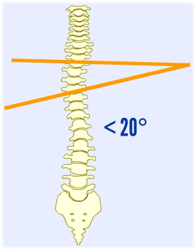
Cobb angle = 11° - 19°
1. Regular follow-up for monitoring curve progression during puberty
Scoliosis may progress rapidly during puberty and become stable in later stage of growth [3]. Mild scoliosis should be managed with regular examinations and exercises.
2. Regular exercises (view more…)
Regular stretching and strengthening exercises can reduce muscle stiffness by keeping the connective fibers of ligaments and tendons flexible. Exercise can also improve mobility and decrease muscle imbalance, hence, reducing the chance of injury and back pain. With regular exercises, a good posture can also be maintained [4,5].

Stretching exercise
Moderate case (Cobb angle = 20° - 45°)
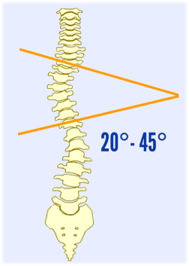
Cobb angle = 20° - 45°
1. Orthotic treatment (Bracing) for adolescent with scoliosis
The aim of orthotic treatment (bracing) is to reduce scoliosis progression when the spinal curvature is between 20° and 45°. Orthosis (brace) applies a corrective force to the spine by compressing the convex part of the curve and relieving on the concave part of the curve in 3-point pressure system [6]. Researches show that the use of bracing significantly reduced the incidence of curve progression and need for surgical management. The orthosis is custom-made and optimized depending on the curve location, curve flexibility, number of curves and vertebral rotation [7,8].
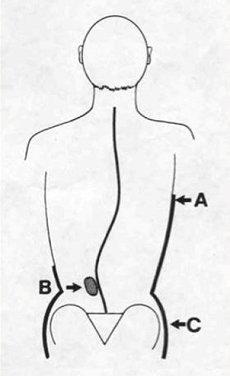
3-point pressure system
There are several types of brace commonly used for treating AIS:
Daytime Orthoses
Cervico-thoraco-lumbo-sacral orthosis (CTLSO) is indicated for the curves with apex at T7 or above. The first CTLSO named Milwaukee brace was developed in the 1940s [9]. It has a rigid metal structure to be worn externally over clothing. Due to its unappealing features, it is rarely used nowadays [10]. However, it can be useful in higher curve deformities at the thoracic or cervical region.
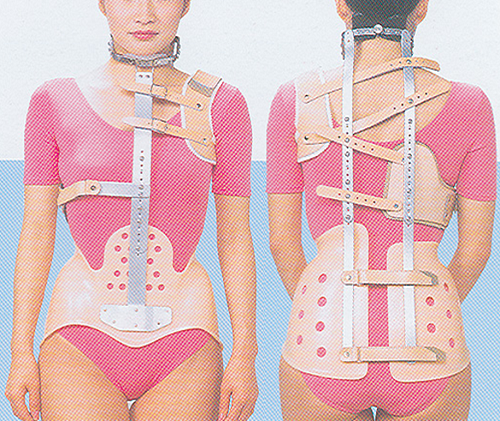
CTLSO (Milwaukee brace)
Thoraco-lumbo-sacral orthosis (TLSO) (e.g. Boston Brace or Wilmington Brace) is indicated for the curves with apex at T8 or below, such as low thoracic, thoracolumbar or lumbar curve. TLSO is made of light plastic material, which can be worn underneath patient’s clothing. They have become the most common orthotic treatment nowadays due to their high level of acceptance and effectiveness of treating scoliosis [11].
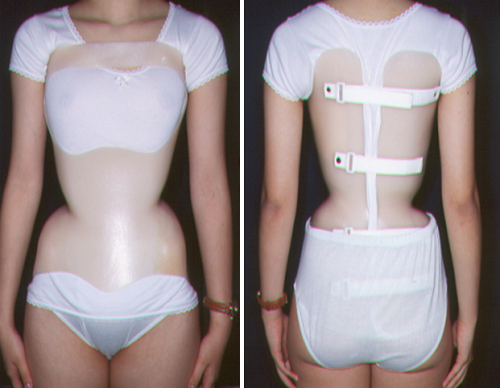
TLSO
Nighttime Orthoses
Charleston bending brace / Providence brace: These two types of thoraco-lumbo-sacral orthosis (TLSO) were developed in 1979 and 1992 respectively. They are suitable for patients with scoliosis curve apex below T7. Nighttime orthoses are to be worn for 8-10 hours, the former design places the body in an over corrected position while the latter design applies strategic forces to control the curves. These night-time braces should be worn until the spine is fully developed [12]. The brace should be reviewed by health professionals every 4 to 6 months. Both designs have similar effect with daytime brace in treating scoliosis in some cases [13,14].

TLSO (Charleston brace)

TLSO (Providence brace)
2. Physiotherapy
Physiotherapy is one of the therapeutic interventions in managing AIS [15-17]. This consists of a range of muscle stretching and strengthening exercises to reduce the effect of muscle imbalance and help maintaining a good posture. The therapy is conducted by physiotherapist and usually in combination with bracing in moderate cases.

Severe case (Cobb angle > 45°)
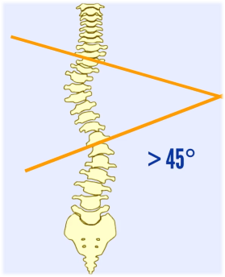
Cobb angle > 45°
1. Surgical treatment
Patients with a Cobb angle larger than 45° should consider spinal fusion surgery to reduce the degree of spinal deformity and reduce the progression of scoliosis. To correct the spinal curvatures, metal rods or implants are placed to realign the spine to allow vertebrae to fuse together into a single bony structure. Post-operatively, patients will be discharged from hospital after 3 to 6 days and they should be able to return to school 3 to 4 weeks after surgery. Normal activities can be resumed in 3 to 6 months after surgery [18,19].
Reference
-
SRS. "Scoliosis Research Society." https://www.srs.org/patients-and-families/common-questions-and-glossary/frequently-asked-questions/treatment-and-coping.
-
H.-R. Weiss, S. Negrini, M. Rigo, T. Kotwicki, M. C. Hawes, T. B. Grivas, T. Maruyama, and F. Landauer, "Indications for conservative management of scoliosis (guidelines)," Scoliosis, vol. 1, no. 1, p. 5, 2006.
-
S. Weinstein and I. Ponseti, "Curve progression in idiopathic scoliosis," The Journal of bone and joint surgery. American volume, vol. 65, no. 4, pp. 447-455, 1983.
-
A. Gruca, "The pathogenesis and treatment of idiopathic scoliosis: a preliminary report," JBJS, vol. 40, no. 3, pp. 570-584, 1958.
-
V. Akuthota, A. Ferreiro, T. Moore, and M. Fredericson, "Core stability exercise principles," Current sports medicine reports, vol. 7, no. 1, pp. 39-44, 2008.
-
R. Fernandez-Feliberti, J. Flynn, N. Ramirez, M. Trautmann, and M. Alegria, "Effectiveness of TLSO bracing in the conservative treatment of idiopathic scoliosis," Journal of pediatric orthopedics, vol. 15, no. 2, pp. 176-181, 1995.
-
SRS. "Scoliosis Research Society." https://www.srs.org/patients-and-families/conditions-and-treatments/adolescents.
-
A. Howard, J. G. Wright, and D. Hedden, "A comparative study of TLSO, Charleston, and Milwaukee braces for idiopathic scoliosis," Spine, vol. 23, no. 22, pp. 2404-2411, 1998.
-
K. J. Noonan, S. L. Weinstein, W. C. Jacobson, and L. A. Dolan, "Use of the Milwaukee brace for progressive idiopathic scoliosis," JBJS, vol. 78, no. 4, pp. 557-67, 1996.
-
F. C. Wickers, W. H. Bunch, and P. M. Barnett, "Psychological factors in failure to wear the Milwaukee brace for treatment of idiopathic scoliosis," Clinical Orthopaedics and Related Research, no. 126, pp. 62-66, 1977.
-
J. E. Lange, H. Steen, and J. I. Brox, "Long-term results after Boston brace treatment in adolescent idiopathic scoliosis," Scoliosis, vol. 4, no. 1, p. 17, 2009.
-
R. S. Fayssoux, R. H. Cho, and M. J. Herman, "A history of bracing for idiopathic scoliosis in North America," Clinical Orthopaedics and Related Research®, vol. 468, no. 3, pp. 654-664, 2010.
-
A. Simony, I. Beuschau, L. Quisth, S. M. Jespersen, L. Y. Carreon, and M. O. Andersen, "Providence nighttime bracing is effective in treatment for adolescent idiopathic scoliosis even in curves larger than 35," European Spine Journal, vol. 28, no. 9, pp. 2020-2024, 2019.
-
R. Gepstein, Y. Leitner, E. Zohar, I. Angel, S. Shabat, I. Pekarsky, T. Friesem, Y. Folman, A. Katz, and B. Fredman, "Effectiveness of the Charleston bending brace in the treatment of single-curve idiopathic scoliosis," Journal of Pediatric Orthopaedics, vol. 22, no. 1, pp. 84-87, 2002.
-
H. Berdishevsky, V. A. Lebel, J. Bettany-Saltikov, M. Rigo, A. Lebel, A. Hennes, M. Romano, M. Białek, A. M’hango, and T. Betts, "Physiotherapy scoliosis-specific exercises–a comprehensive review of seven major schools," Scoliosis and spinal disorders, vol. 11, no. 1, p. 20, 2016.
-
S. Negrini, C. Fusco, S. Minozzi, S. Atanasio, F. Zaina, and M. Romano, "Exercises reduce the progression rate of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature," Disability and rehabilitation, vol. 30, no. 10, pp. 772-785, 2008.
-
H.-R. Weiss, G. Weiss, and H.-J. Schaar, "Incidence of surgery in conservatively treated patients with scoliosis," Pediatric Rehabilitation, vol. 6, no. 2, pp. 111-118, 2003.
-
S. Yadla, M. G. Maltenfort, J. K. Ratliff, and J. S. Harrop, "Adult scoliosis surgery outcomes: a systematic review," Neurosurgical focus, vol. 28, no. 3, p. E3, 2010.
-
E. R. Westrick and W. T. Ward, "Adolescent idiopathic scoliosis: 5-year to 20-year evidence-based surgical results," Journal of Pediatric Orthopaedics, vol. 31, pp. S61-S68, 2011.